
My response to Tracy Beth Høeg's response to Denis Rancourt et al.!
A data driven review of the latest article that critically discusses the claim of 17M vaccine deaths.

In a new guest post by Tracy Beth Høeg on Dr. Bhattacharya & Ray Arora’s Substack “The Illusion of Consensus”, the Tracy critically responds to the “17M vaccine death claims” as raised awareness by Brett Weinstein on Tucker Carlsons show.

In this rapid-response, I will discuss the major points raised by Tracy, whom I respect and applaud for her critical response to the authoritarian driven & completely failed COVID-19 overreach. I do agree with many of her points raised in the article, and I will mostly only focus on the areas where I disagree.
“Basic Math / Sanity Check”
Tracy starts her article, by doing a quick sanity check, she argues, that at the proposed “vaccine mortality rate”, Denmark should have seen “about 15,000 excess deaths”.
Let’s look at mortality data from Mortality.Watch, which I started developing beginning of 2023. Mortality.Watch is free & open-source, and relies on the R package fable for statistical analysis and predictions. Mortality.Watch uses a linear regression of length n years. For each jurisdiction, period of time and metric, pre-pandemic data is back tested to choose the baseline length n with the lowest root mean squared error (RMSE) for a three to ten-year period of a four-year forecast. The exact chart URL can be retrieved by scanning the QR code in the top right of each chart.
Here are the crude deaths for Denmark with a 2011-2019 baseline:

Thus resulting in the following Excess Deaths:

Since there were essentially none in 2020, cumulative this model produces around 10,000 excess deaths in total for 2021-2023.

So this would only account for 2/3 of her (very simplified) calculated excess deaths.
However, there are at least two factors that this misses:
Taking into account the uncertainty that’s involved with the baseline model, we can calculate the cumulative number, including 95% prediction intervals. This is not supported on Mortality.Watch yet, but I have calculated the cumulative total in R:
Actual deaths: 229,491, Expected Deaths: 219,366, 95%PI[211,248,227,485]
Excess deaths: 10,125, 95%PI[2,006, 18,243]
As you can see, this model produces an upper limit of 18k excess deaths, so this would be in-line with the 15k estimate!
Denmark is an extremely highly developed country:
Ranking 6th of all countries by Human Development Index (HDI)
Ranking consistently in the top 20 by health status and health care index!
Thus, it is to be expected that the underlying health status of the Danish population is likely much more healthy than poor regions of the US, or Eastern Europe!
For a complete picture, here are the crude and age standardized figures:

It is evident, that excess mortality only rose starting in mid 2021, thus after the COVID-19 vaccine intervention. Now there are clearly some other likely seasonal effect accruing, but we can see that there’s clearly an extraordinary rise after vaccination. With a “highly-effective vaccine” much milder “variants” this is rather implausible to be due to COVID-19.

Excess mortality study by Ioannidis et al.
The study by Ioannidis & Levitt, has some limitations, as it uses a simple 3y average without trend, thus leading to systemic underestimation of excess deaths with a declining trend.
Additionally, after a period of high mortality, a period with lower mortality should be expected! An analysis of excess mortality before and after vaccination shows, that excess mortality is ongoing, and many countries have not returned to pre-pandemic levels!
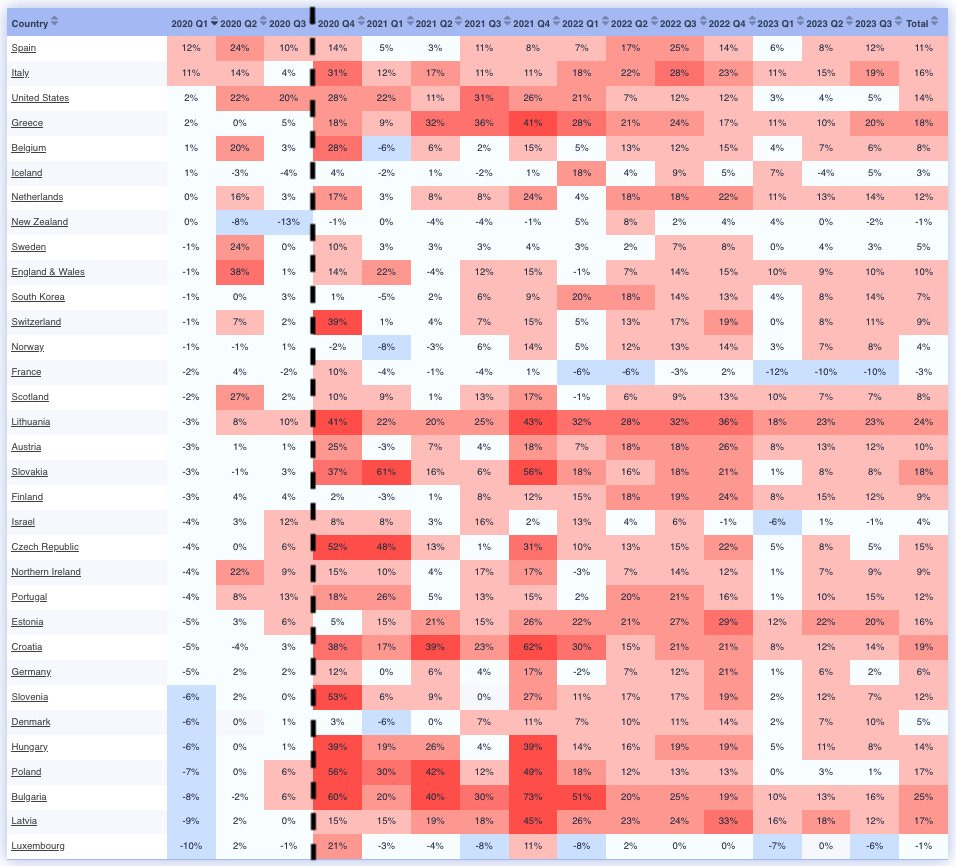
Next, Tracy claims: “Countries with relatively high vaccination rates didn’t have any”. While there are some countries, that in sum, appear to have no excess mortality, she is again forgetting about the uncertainty. A closer look reveals, that many of those “low excess countries” saw some excess mortality in 2022, specifically when you look at the upper limit of the 95% PI.

Again, these countries have also typically a very good health status.
Rancourt et al.
Now Tracy criticizes that Rancourt et al., conclude that a “definite causal link” has been shown. While I agree with Tracy, that these epidemiological charts cannot show that - I think Rancourt is operating under the null-hypothesis that no efficacy has even been shown against all-cause illness, hospitalization or mortality for the COVID-19 vaccines and thus operating under the assumption of negative VE (only toxicity).
Countries in the Southern Hemisphere typically rank lower in health index, thus more excess deaths may be expected by any intervention.
My “before vs. after" intervention” analysis of the top 20 most vaccinated countries shows increasing excess mortality after the intervention in each country, which again, is inconsistent with a “highly effective & safe vaccine” and much lower variant mortality.
Next, Tracy mentions, that Rancourts time series charts “Do not clearly correspond to the vaccine rollout”. However, it is noteworthy that under the toxicity hypothesis, mostly older/frail would be affected, that were typically vaccinated at the beginning.
Let’s also not forget, that there are many other factors mixed into these all-cause charts, such as seasonal excess patterns.
Dr. Morris et al.
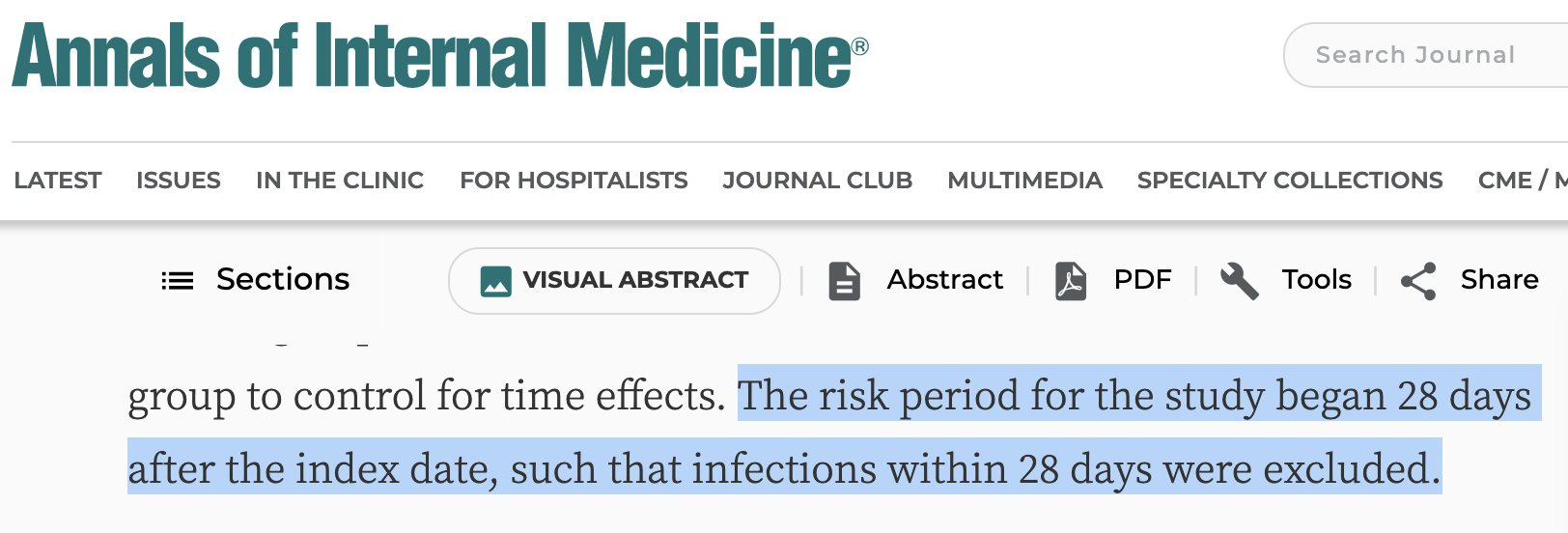
Then Tracy mentions claims of Dr. Morris who entirely blames excess deaths on unvaccinated people.
Not only is his entire study extremely biased, as it looks only at COVID-19 attributed deaths and not all-cause, but it also excludes people up to 28 days after vaccination.
Moreover, there may be two type of “vaccine deaths”:
Immediate, which may occur <14 days after vaccination, and could possibly vastly misattributed as COVID-19.
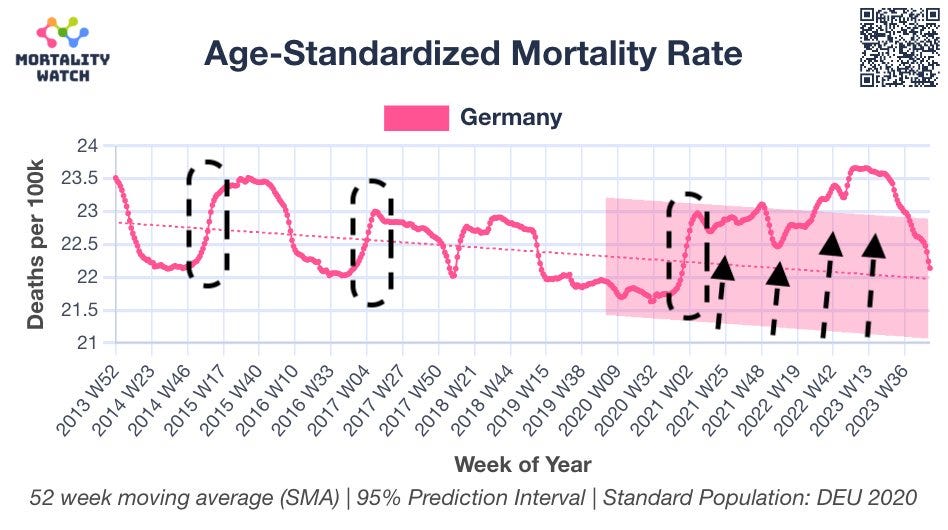
Systemic long-term
“Vaccine deaths” may not be immediate (only in the very frail) but may be systemic over time, thus causing a higher level of mortality. This may be observed in Germany, where you can see normal seasonal effect encircled, and a systemic increase after intervention:
Stabell Benn et al.
Lastly, Tracy mentions the study of Stabell-Benn et al. which is a meta study of the original RCT’s. Here Tracy claims that no increase was observed, however that is strictly speaking not accurate, as for mRNA vaccines - a 3% increase, however not stat. sign., was observed.

302 Confirmed Vaccine Death in Germany
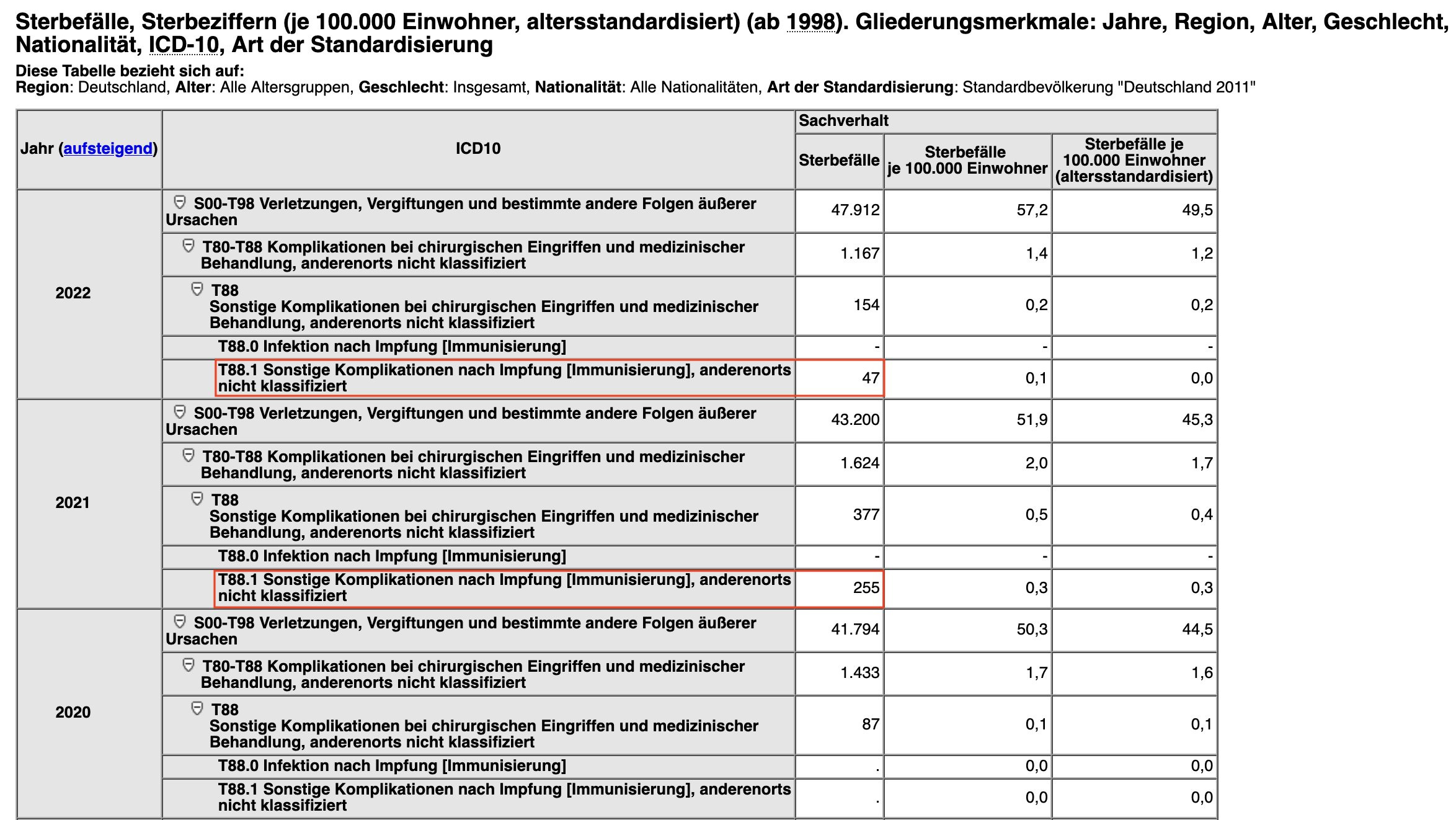
Also noteworthy, that the German federal statistical office has confirmed 302 deaths by COVID-19 vaccination. Of course, they tried to hide the data in the ICD-10 category for “T88.1: Other complications following immunization, not elsewhere classified”, but historic analysis shows that there were no deaths in that category before 2020, thus making it almost certainly causal to COVID-19 vaccination.
At 64.9% vaccinated population, this brings the risk to about 1:180,000 vaccinated as the lower limit.
Conclusion
Rancourt's estimate of 17M excess deaths are definitely within a possible range.
Possible “vaccine deaths” may greatly vary based on age and underlying health status.
The ongoing systemic hiding of relevant data by authorities, which does not allow proper analysis, is highly concerning.
Not a single country will willfully disclose their record level data. I wonder why??? Hmmmm
EXCELLENT response and analysis- far more factual/accurate, balanced, and to-the-point than almost all of what I've seen so far. Thank you very much for this.