
Does Measles Vaccination Reduce Cases? A Deep Dive Into WHO Data
An analysis of 25 years of global measles data reveals patterns inconsistent with vaccine efficacy claims

I analyzed the relationship between measles vaccination coverage and reported cases using official WHO data from 2000-2024. The results were surprising: the data doesn’t clearly support the claim that vaccines reduce measles cases.
Before you dismiss this as “anti-vax,” read the methodology and the numbers. This is a data analysis, not an opinion piece.
TL;DR
WHO’s own data doesn’t clearly support vaccine efficacy for measles. The correlations that exist can be explained by confounding.
The Data
I used two datasets from the WHO Global Health Observatory:
- Measles cases (indicator WHS3_62)
- MCV1 vaccination coverage among 1-year-olds (indicator WHS8_110)
- Population data from mortality.watch
The analysis covers all 6 WHO regions: Africa (AFR), Americas (AMR), Eastern Mediterranean (EMR), Europe (EUR), South-East Asia (SEAR), and Western Pacific (WPR).
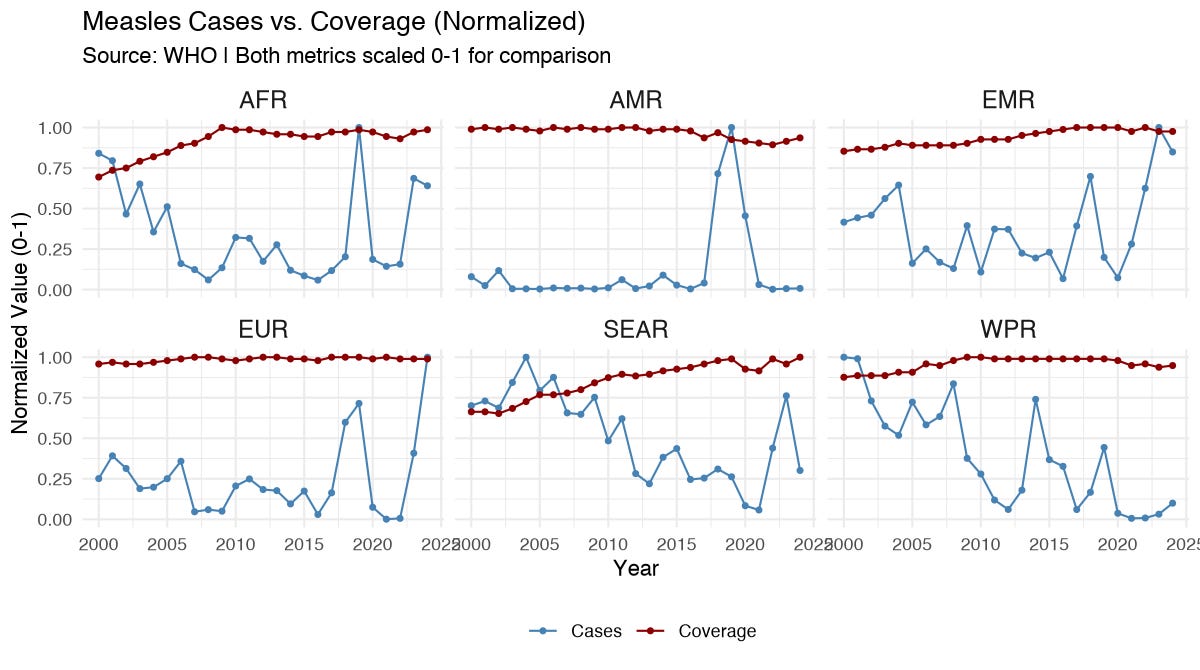
Finding #1: Only Half the Regions Show Any Correlation
If vaccines reduce measles, we’d expect a negative correlation between coverage and cases everywhere. Instead:
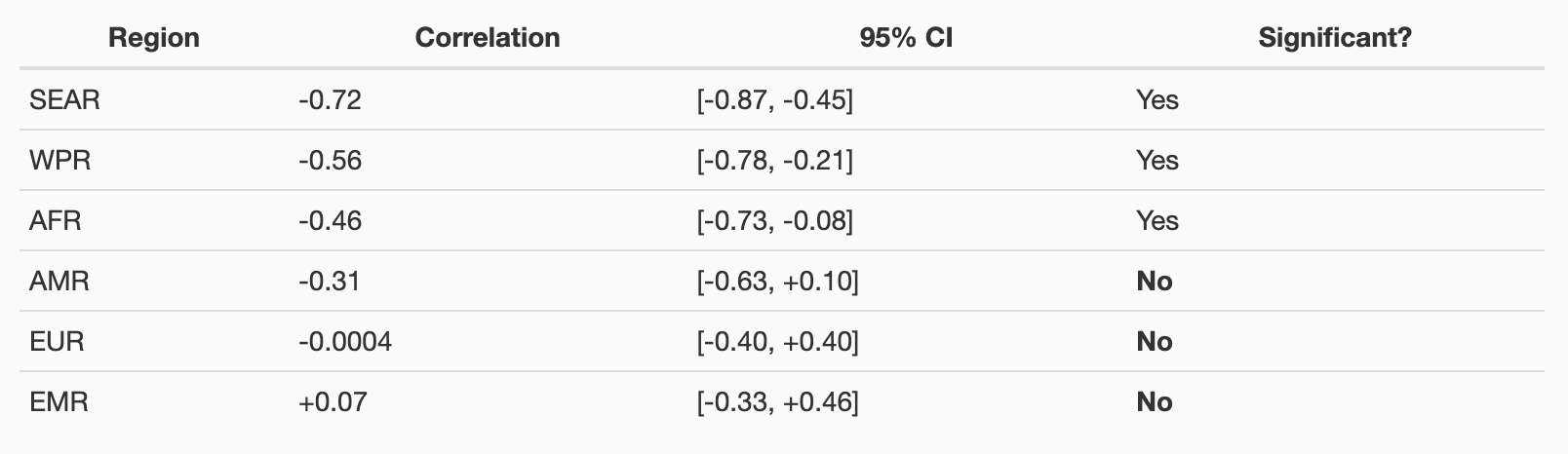
Three regions (Americas, Europe, Eastern Mediterranean) show no statistically significant correlation between vaccination and cases. Europe’s correlation is essentially zero (-0.0004).
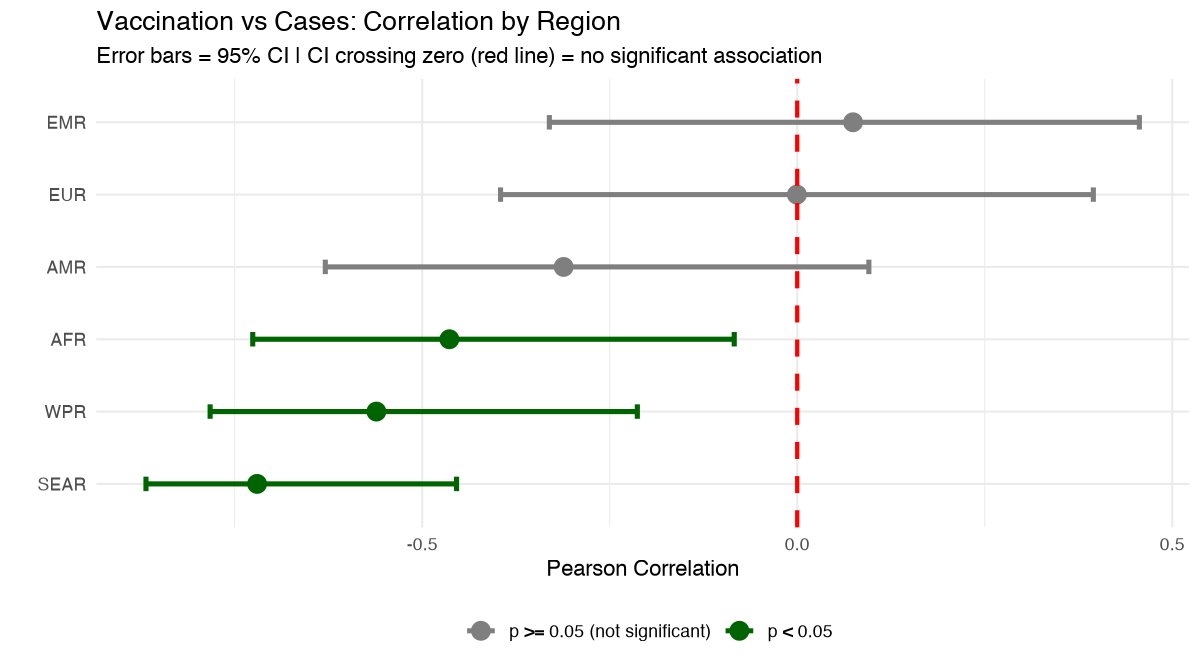
Finding #2: The Confounding Pattern
Here’s what’s telling: the correlations appear only in developing regions (Africa, South-East Asia, Western Pacific) and are absent in developed regions (Europe, Americas).
This is exactly what you’d expect from confounding, not causation.
If vaccines caused the decline:
- We’d see negative correlations in ALL regions
- Europe and Americas have high vaccination rates - the effect should be visible
If development caused the decline:
- Developing regions: Sanitation, nutrition, healthcare ALL improved alongside vaccination programs
- Developed regions: These factors were already stable - no correlation appears
👉 The pattern fits confounding perfectly.
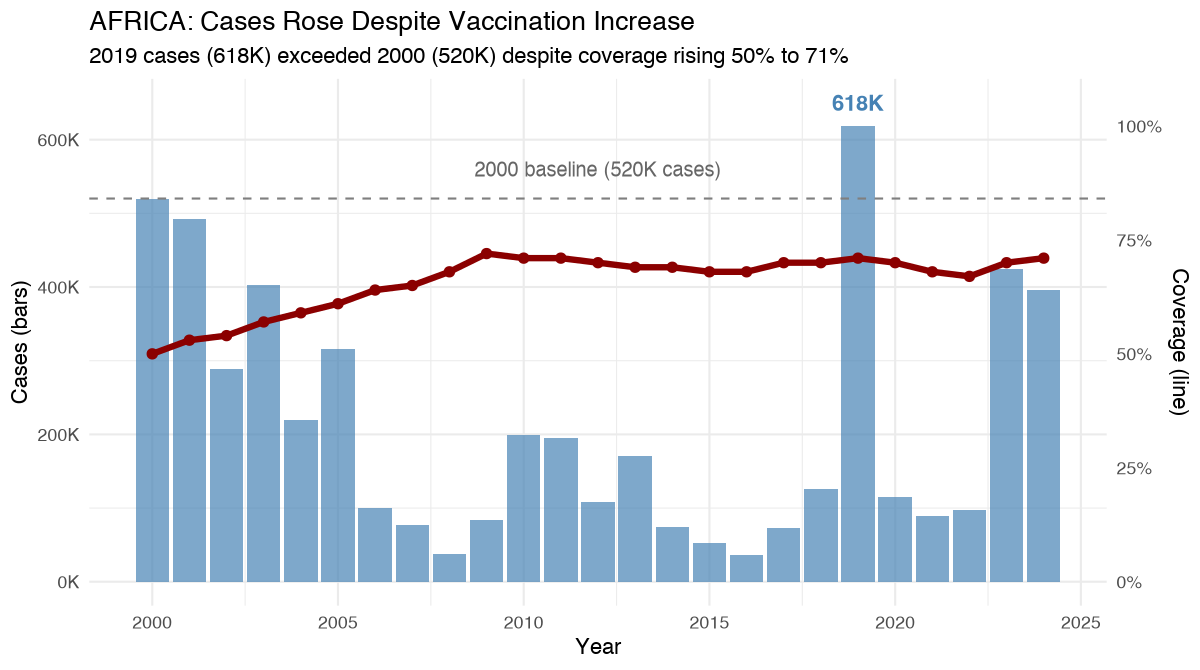
Finding #3: The Africa Anomaly
Africa provides the clearest test case. Coverage increased substantially over 24 years:
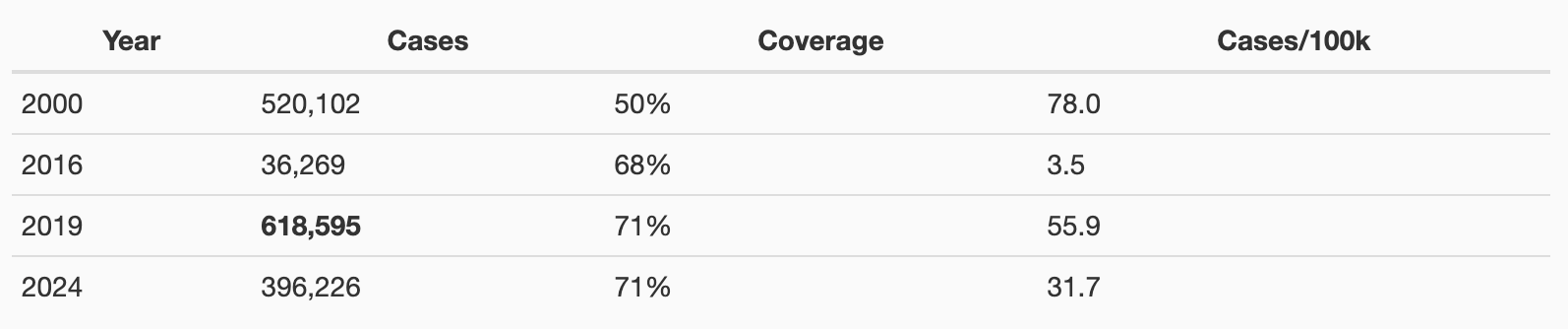
Cases in 2019 exceeded 2000 levels despite coverage rising from 50% to 71%.
If vaccines worked, this shouldn’t happen. You can’t have 21 percentage points more coverage and end up with more cases than you started with.
Finding #4: Year-Over-Year Analysis Shows Nothing
I tested whether years with increasing coverage correspond to years with decreasing cases:
Regression: Cases_change ~ Coverage_change
Slope: +4.12 (positive, not negative!)
p-value: 0.89 (nowhere near significant)
95% CI: [-52.4, +60.7]
R-squared: 0.00015 (essentially zero)
There is no detectable relationship between coverage changes and case changes. Years when vaccination increased were not associated with fewer cases.
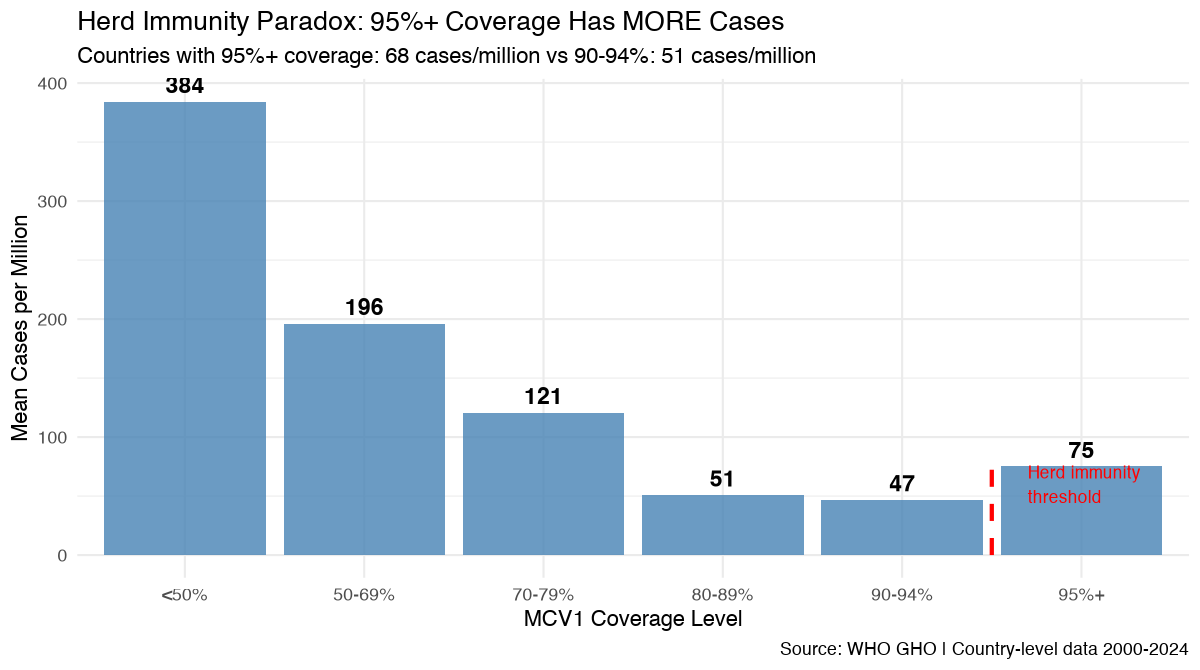
Finding #5: Herd Immunity Threshold Not Observed
The theory says measles requires 92-95% coverage for herd immunity. Above this threshold, cases should plummet.
Reality:
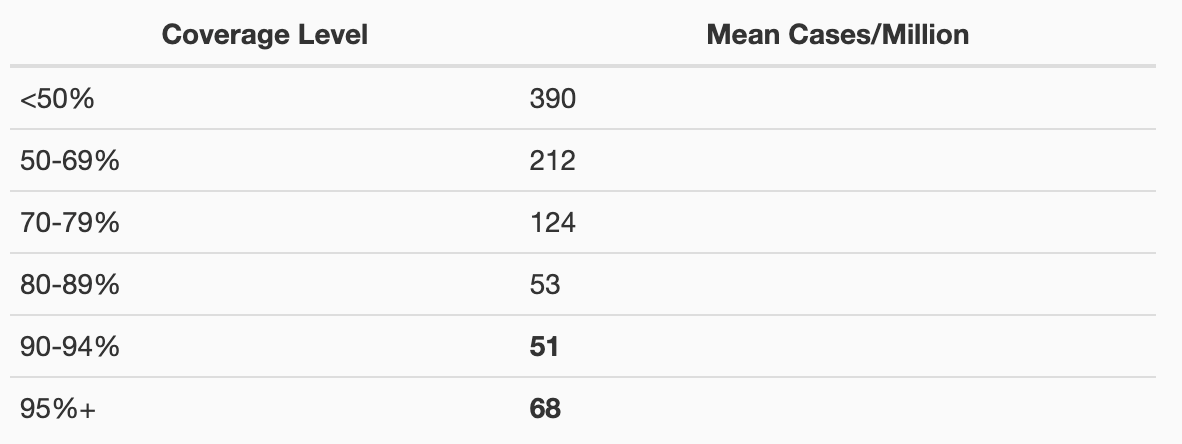
Countries with 95%+ coverage have HIGHER case rates than 90-94% coverage.
Recent high-coverage “outbreaks”:
- Samoa (96% coverage): 27,341 cases per million
- Tonga (99% coverage): 2,130 cases per million
- Kyrgyzstan (96% coverage): 1,125 cases per million
The expected threshold effect simply isn’t visible in the data.
Finding #6: Lag Analysis Doesn’t Help
Maybe vaccines take time to show effect? I tested if coverage predicts cases 1-3 years later:

Africa’s correlation gets weaker with longer lags. This is the opposite of what you’d expect if vaccines caused a delayed reduction.
What This Analysis Shows
1. Temporal correlation exists between vaccination and case decline in developing regions
2. No correlation exists in developed regions despite high coverage
3. Pattern consistent with confounding by development (sanitation, nutrition, healthcare)
4. Africa anomaly - cases exceeded baseline despite coverage nearly doubling
5. No year-over-year relationship (p=0.89)
6. Herd immunity threshold not observed - 95%+ coverage countries still have major outbreaks
Limitations
To be clear about limitations:
- This cannot prove vaccines don’t work
- This cannot prove vaccines do work
- Ecological data cannot establish causation
- This doesn’t tell us what would have happened without vaccination
Alternative Explanation
The pattern is more consistent with:
👉 “Development reduces measles through improved sanitation, nutrition, and healthcare. Vaccination programs are part of development initiatives. The correlation is spurious.”
Than with:
👉 “Vaccines reduce measles cases.”
If vaccines were the causal factor, we’d expect to see the effect in ALL regions, not just those undergoing rapid development.
Conclusion
The WHO’s own data doesn’t clearly support the claim that measles vaccination reduces cases. The correlations that exist can be explained by confounding. The Africa data directly contradicts efficacy claims. The herd immunity threshold isn’t visible.
This doesn’t mean vaccines definitely don’t work. But it does mean the ecological evidence cited to support their efficacy is weak and potentially spurious.
To properly establish efficacy requires double blinded randomized placebo controlled trials, case-control studies, or natural experiments - not ecological time-series correlations, that don’t exist.
Source & Code
WHO Global Health Observatory, mortality.watch
WHO is 10,000% controlled by gates and big pharma and is a loyal servant to germ theory. Therefore, I cannot trust their data any more than the data from the HHS. I know for certain that I have had no vaccines in about 50 years and no flu in over 30. That is all the data I need to say NO to vaccines and drugs.
The CDC is built to look at this same data….supposedly!…yet they are clueless….Why has the Trump Admin not received such deep dive info by the “experts” there??….Time to either get accurate and deep dive or we need to remove all and repopulate it with pro-citizen people….either they are with improving a needed or not vac injections and all the toxins within the vac.